
By Editor
February 25, 2026
Itraconazole Cream – Itraconazole is a triazole antifungal used widely as an oral medication for skin, nail and systemic fungal infections. Topical itraconazole creams and formulations do exist and have been the subject of development and some clinical research; they are available in some markets (and in combination products) but regulatory approval and product availability vary by country. Topical use is most relevant for localized skin fungal infections; oral itraconazole remains the standard for deeper or widespread infections and for nail (onychomycosis) disease. Always check with a healthcare professional before starting treatment.
What is itraconazole?
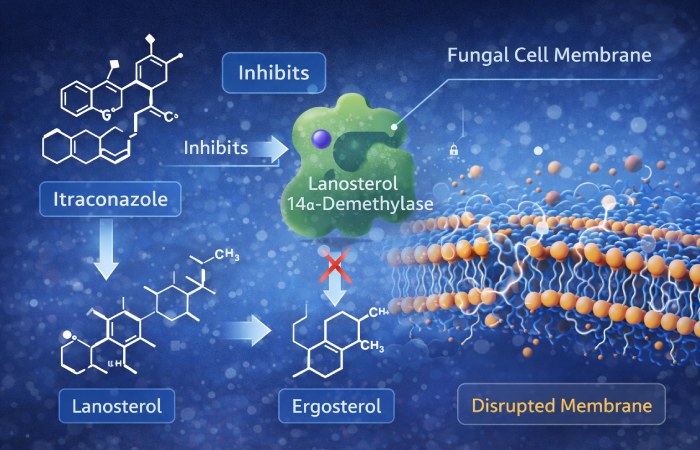
Itraconazole is an antifungal drug from the triazole family. It works by blocking the fungal enzyme lanosterol 14-α-demethylase and thereby preventing ergosterol synthesis — an essential component of fungal cell membranes. Disrupting ergosterol production weakens the fungal cell membrane and stops fungal growth. This is the same broad mechanism used by other azoles.
Itraconazole is most commonly used as an oral medicine (capsules or oral solution) and as an intravenous formulation where needed; oral dosing and indications are well established for conditions like onychomycosis and systemic fungal infections. The oral route requires attention to interactions, liver safety, and cardiac precautions.
So – does “itraconazole cream” exist?
Yes — topical itraconazole formulations have been developed and topical creams containing itraconazole (typically 0.25–1% or in combination with other antifungals) are marketed in some countries and produced by several manufacturers. In addition, topical development work (including dose-finding studies) has been published. However, the regulatory status differs by country: topical itraconazole is not a universally FDA-approved topical product in the US (oral/IV itraconazole is the established FDA-approved form); some topical products on the market are regionally approved or sold under local licences. Always check local product labels and regulatory listings.
Why consider topical itraconazole?
Topical antifungals are commonly first-line for localized superficial fungal skin infections (tinea corporis, tinea cruris, tinea pedis, pityriasis versicolor, cutaneous candidiasis). Advantages of a topical formulation are:
- Direct delivery to the affected skin → high local concentrations
- Minimal systemic exposure compared with oral therapy (usually)
- Fewer systemic drug-drug interactions and systemic side effects
- Useful for patients who cannot take oral azoles
Topical itraconazole was explored to combine the azole’s broad antifungal coverage with topical delivery advantages. Dose-finding and formulation studies (including liquid-crystal and cream bases) have looked promising for skin penetration and local activity.
Evidence summary — topical itraconazole: what clinical studies show
- A small, early dose-finding placebo-controlled study tested 0.25% and 0.5% itraconazole creams applied once daily and used skin surface culture methods to measure antifungal effect — results supported local antifungal activity and helped guide topical dose selection. This is early clinical evidence that topical itraconazole can act locally against fungal colonization.
- More recent pharmaceutical formulation studies and product development papers (including liquid crystal and oil-based creams) report good in-vitro antifungal zones of inhibition and measurable skin penetration. These studies support the feasibility of topical delivery but are not the same as large randomized clinical outcome trials.
- In several comparative clinical studies of oral antifungals for dermatophytosis (skin ringworm), itraconazole (oral) has been compared with terbinafine (oral) and other systemic regimens. Those studies relate to systemic therapy, not topical, but they show itraconazole’s clinical role for more extensive infections. For localized superficial disease, topical therapy (classically clotrimazole, terbinafine, or eberconazole in some regions) remains standard — topical itraconazole can be an option where it’s available and supported by product labelling and prescriber judgment.
Bottom line on evidence: academic and manufacturer studies show topical itraconazole has antifungal activity and is feasible as a cream formulation, and small controlled studies exist. Large, multicenter randomized outcome trials comparing topical itraconazole with standard topical agents are limited. Use should therefore be guided by local approvals, manufacturer instructions, and clinical judgement.
How topical itraconazole is typically used
Important: The instructions below describe general, commonly used topical treatment patterns for superficial fungal infections. Always follow the product label and your prescribing clinician.
- Indications (where topical therapy is appropriate): localized tinea corporis (ringworm), tinea cruris (groin), limited tinea pedis (athlete’s foot), pityriasis versicolor, and cutaneous candidiasis — depending on product labelling.
- Typical frequency: topical antifungal creams are often applied once or twice daily to the affected area for 2–4 weeks or until clinical and (if required) mycological cure. For itraconazole cream, some product inserts suggest twice daily application for several weeks — follow label guidance.
- Application tips: wash and dry the area, apply a thin layer covering the lesion and a small margin of surrounding skin, wash hands after application (unless hands are being treated).
- Duration: continue as advised by your clinician or the product instructions — premature stopping increases relapse risk.
Topical vs oral itraconazole — when to choose which

- Use topical (including topical itraconazole where available) for small, localized, superficial infections. Topical therapy usually suffices for limited tinea corporis/cruris/pityriasis versicolor and for mild cutaneous candidiasis.
- Use oral itraconazole when infections are widespread, involve nails (onychomycosis), hair follicles, or are recurrent, chronic, or refractory to topical therapy, or when systemic therapy is specifically indicated (e.g., tinea unguium). Oral itraconazole dosing is proven for onychomycosis and systemic fungal disease; the oral route requires clinician oversight due to liver and cardiac cautions.
Safety and interactions — topical vs systemic
Topical safety: topical antifungals (including itraconazole cream) generally have fewer systemic side effects because systemic absorption is low. Local adverse effects can include irritation, redness, burning, or allergic dermatitis. Rare systemic absorption with extensive application or broken skin is possible, so caution in very large surface-area use or compromised skin.
Systemic (oral) safety highlights — reasons to consult a clinician before oral itraconazole:
- Hepatotoxicity: oral itraconazole can cause liver enzyme elevations and, rarely, severe liver injury. Monitor LFTs when on systemic therapy as directed.
- Cardiac effects: itraconazole can cause negative inotropic effects and has been associated with congestive heart failure in some patients. Patients with heart failure or cardiac disease generally should not take oral itraconazole.
- Drug interactions: itraconazole is a strong inhibitor of CYP3A4 and interacts with many commonly used medications (statins, certain antiarrhythmics, benzodiazepines, some antivirals, etc.). This risk applies to oral therapy and not typically to topical use. Always check drug interactions before starting oral itraconazole.
Practical safety rule: topical itraconazole reduces systemic risk compared with oral therapy, but if you have liver disease, heart disease, or take interacting drugs, discuss options with your clinician. For extensive disease, oral therapy may be necessary despite systemic risks — that decision should be clinician-led.
Special situations & cautions
- Pregnancy & breastfeeding: systemic itraconazole is typically avoided in pregnancy unless clearly needed; topical products should still be discussed with an obstetric clinician.
- Children: use pediatric dosing recommendations if available; many topical antifungals are used in children but check product labelling.
- Allergy: if you have prior allergy to azoles, avoid itraconazole.
- Large area application: avoid applying large amounts of topical formulation over extensive body surface area without medical advice because of possible systemic absorption.
Practical tips for patients and clinicians
- If the product is not available locally, ask about alternative topical antifungals (clotrimazole, miconazole, terbinafine, eberconazole) which are widely used and effective for superficial tinea and candidal skin infections.
- For hair or nail fungal infections, topical therapy is usually not sufficient — systemic therapy is typically required.
- If skin lesions do not improve after the recommended topical course (or worsen), seek re-evaluation — confirm diagnosis (KOH microscopy/culture) and consider systemic therapy if indicated.
Frequently asked questions (FAQ)
Q: Is itraconazole cream better than clotrimazole or terbinafine cream?
A: There’s no simple “better” answer. Terbinafine and azole topical agents (clotrimazole, miconazole) are established, inexpensive, and effective for many tinea infections. Topical itraconazole has promising activity and some supportive studies, but large comparative outcome trials are limited; local availability and clinician preference influence choice.
Q: Will topical itraconazole work for nail fungus?
A: Topical creams rarely penetrate thick nail plates well; nail fungal infections usually need oral therapy (itraconazole oral, terbinafine oral) or medicated nail lacquers specifically designed for nail penetration.
Q: Are topical itraconazole products safe to buy online?
A: Be careful: product quality and regulatory approvals vary. Only purchase from reputable suppliers and check local approvals. Avoid unverified online vendors or imported medications without clear labelling.
Q: How long until the rash improves?
A: Many superficial fungal rashes improve within 1–2 weeks of effective topical therapy, but continue the full course as recommended (often 2–4 weeks) to reduce relapse. Nail infections require months of therapy.
References — five load-bearing sources used
- Itraconazole — StatPearls (NCBI Bookshelf) — dosing, formulations, pharmacology.
- Antifungal Ergosterol Synthesis Inhibitors — mechanism overview (StatPearls / NCBI).
- Itraconazole Monograph & Warnings — Drugs.com monograph (safety/interaction details).
- MedlinePlus — Itraconazole drug information (serious warnings including cardiac, liver).
- Dose-finding and topical itraconazole trial — J Med Vet Mycol (1995) — placebo-controlled study with 0.25% and 0.5% itraconazole cream.
(Additional formulation research and product pages cited above include PubMed formulation studies and regional product listings).
Final notes / clinical caution
- This article is informational and not a prescription. Do not start or stop antifungal therapy without consulting a healthcare professional.
- If you have liver disease, heart problems, or take multiple medicines, oral itraconazole requires clinician supervision — topical therapy may reduce systemic risk but check product labels.
