Pre & Probiotic Capsules – Prebiotics (non-digestible fibers) feed beneficial gut microbes while probiotics are live microorganisms that can temporarily alter gut flora. Taken as capsules, probiotics have the best evidence for preventing antibiotic-associated diarrhea and helping some people with IBS and acute infectious diarrhea; prebiotics support growth of helpful bacteria and show promise for metabolic and immune benefits. Not all strains or products work the same — benefits are strain- and dose-specific — and people who are severely ill or immunocompromised should use caution. See dosing, how to choose a quality product, proven uses, and common safety notes below.
What are prebiotics and probiotics?
- Probiotics are live microorganisms (usually bacteria such as Lactobacillus or Bifidobacterium, or yeast like Saccharomyces boulardii) that — when given in adequate amounts — may confer a health benefit. As capsules they deliver concentrated, targeted strains.
- Prebiotics are non-digestible food components (types of fiber and resistant starches such as inulin, fructooligosaccharides) that selectively feed beneficial gut bacteria and increase production of short-chain fatty acids (SCFAs) that help gut health. They are commonly available as powders or capsules.
Together (probiotic + prebiotic), they’re often called synbiotics — the idea is the prebiotic helps the probiotic survive and thrive. Research shows that prebiotics are non-digestible fibers that feed beneficial gut bacteria and are fermented by gut microbes to produce metabolites that influence digestive and overall health.
How pre & probiotic capsules work
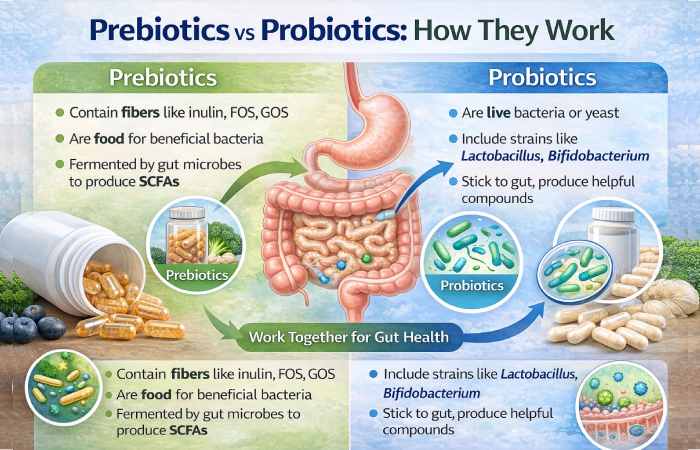
- Probiotics can colonize temporarily (not usually permanently) and interact with your gut lining, immune cells, and resident microbiota. They may: compete with pathogens, produce antimicrobial compounds, strengthen the intestinal barrier, and modulate immune responses.
- Prebiotics reach the colon undigested, where resident beneficial microbes ferment them into SCFAs (acetate, propionate, butyrate) that feed colon cells, reduce inflammation, and influence metabolism and immunity.
Evidence-based uses for probiotic capsules
Important: probiotic effects are strain-specific — one strain’s benefit does not automatically apply to another. Look for products listing the exact strain(s) and clinical studies.
1. Prevention of antibiotic-associated diarrhea (AAD)
Multiple systematic reviews and meta-analyses show probiotics reduce the risk of AAD if taken alongside antibiotics — commonly studied strains include Lactobacillus rhamnosus GG and Saccharomyces boulardii. The pooled evidence indicates a moderate protective effect (e.g., relative risk reductions in meta-analyses), and higher doses (>10 billion CFU/day) often performed better.
2. Acute infectious diarrhea (adults & children)
Probiotics shorten the duration of some acute infectious diarrheas and reduce symptom severity in multiple randomized trials and systematic reviews; effects vary by organism and patient population (viral vs bacterial).
3. Irritable bowel syndrome (IBS)
There is good evidence that certain probiotic strains or combinations can reduce IBS symptoms (abdominal pain, stool irregularity) and improve quality of life — but benefits differ by strain and IBS subtype (IBS-D, IBS-C, etc.). Use of evidence-backed strains (e.g., some Bifidobacterium, Lactobacillus, B. coagulans) for at least 4–8 weeks is typically studied.
4. Traveller’s diarrhea, some forms of constipation, and adjuncts to H. pylori therapy
Meta-analyses show modest reductions in traveler’s diarrhea and possible benefits for some constipation types; probiotics are also used as adjuncts during H. pylori eradication to reduce side effects of therapy and sometimes improve eradication rates.
5. Emerging / tentative areas — mood, cognition, metabolic health
Early trials suggest probiotic supplements may have small benefits for cognition, mood, and some metabolic markers, but the certainty is low and more trials are needed. Treat these as promising but not definitive.
Studies show that fermentation of prebiotic fibers produces short-chain fatty acids such as acetate and butyrate, which support intestinal cells and metabolic health.
Evidence-based uses for prebiotic capsules
- Support growth of Bifidobacteria and related beneficial groups. Clinical studies (and infant formula trials) show prebiotic supplementation can increase beneficial bacteria counts and lower fecal pH (a marker of fermentation).
- Potential benefits for immunity and mineral absorption. Some trials link prebiotics to improved calcium absorption and modest immune effects, but high-quality long-term human data are still limited.
- Role as part of synbiotic approaches. Combining a known probiotic strain with an appropriate prebiotic can increase the chance the probiotic will work, especially when the prebiotic selectively feeds that strain.
Who is most likely to benefit?
- People taking antibiotics (to help prevent AAD) — choose strains with evidence (e.g., S. boulardii, L. rhamnosus GG).
- People with IBS (after checking with their clinician) — use strain(s) with RCT support for IBS.
- Travelers at high risk for traveler’s diarrhea (selected probiotics show modest benefit).
- Those seeking general gut-microbiome support who prefer an evidence-based supplement and eat a fiber-rich diet (pair prebiotics + probiotics for best synergy).
Dosing: practical, evidence-oriented guidelines
- Probiotics (capsules): Commonly used doses range from 1 billion to 50+ billion CFU per day, but many clinical trials showing benefit use >10⁹–10¹⁰ CFU/day depending on strain and condition. For prevention of AAD, meta-analyses suggest doses greater than about 10 billion CFU/day were more effective. Always follow product label or clinician advice.
- Prebiotics (capsules/powders): Typical study doses for inulin, FOS, or GOS range from 2–10 g/day. Start low (1–2 g/day) and increase gradually to avoid gas/bloating.
- Timing: If taking probiotics with antibiotics, separate doses by 2–3 hours to reduce antibiotic killing of probiotic organisms. Continue probiotics for 1–2 weeks after antibiotic course when the aim is to prevent AAD (specific durations vary by trial).
Safety & side effects — what to expect and red flags
- Common effects: Mild, transient gas or bloating when you start a prebiotic or probiotic (usually resolves in days).
- Rare but important risks: In severely ill, hospitalized, or immunocompromised patients, there have been rare reports of probiotics causing bloodstream infections or fungemia (notably with Saccharomyces in vulnerable patients). For these groups, consult a clinician and prefer medical supervision.
- Product quality issues: Supplements are less tightly regulated than medicines. Some products have inconsistent strains or CFU counts. Choose brands with third-party testing and transparent strain documentation.
How to choose a good pre/probiotic capsule product (checklist)
- Strain specificity: Product lists exact strain(s), e.g., Lactobacillus rhamnosus GG (ATCC 53103) — not just genus names.
- Clinical evidence: Look for citations or clinical trials on the product page; prefer strains with RCT support for your target use (e.g., AAD, IBS).
- CFU at end of shelf life: Good manufacturers specify CFU through end of shelf life, not just at manufacture.
- Third-party testing: USP, NSF, or independent lab verification for identity/purity/potency.
- Storage & delivery: Enteric-coated or gastro-resistant capsules and refrigeration (if required) help organisms survive gastric acid. Check label directions.
- Allergens and excipients: Check for dairy, soy, gluten, or other allergens if you have sensitivities.
- Prebiotic composition: For prebiotic capsules, check whether the product contains inulin, GOS, FOS, resistant starch, or other fibers — and the gram amount per serving.
Synbiotics: when to combine pre + probiotic
- A synbiotic intentionally pairs a probiotic strain with a prebiotic substrate that supports that strain (e.g., Bifidobacterium + GOS). Some trials show larger or more consistent effects for synbiotics in stress models and niche clinical uses, but again benefit is strain/prebiotic specific.
Common myths — quick fact checks
- Myth: “One probiotic capsule will permanently fix my gut.” → Fact: Most probiotics colonize temporarily; benefits usually require continued use and are strain-specific.
- Myth: “All probiotics are the same.” → Fact: Not true — species, strain, dose, and formulation matter. Look for human clinical trial support for your condition.
- Myth: “Prebiotics always cause gas.” → Fact: They can cause gas initially — titrating slowly and keeping hydrated lowers side effects.
Practical regimens
These are example regimens commonly used in trials. Discuss with your clinician before starting.
- To help prevent antibiotic-associated diarrhea: Choose a product containing L. rhamnosus GG or S. boulardii at ~10–20 billion CFU/day, start with the first antibiotic dose (or within 48 hours) and continue 1–2 weeks after finishing antibiotics, keeping doses separated by ≥2 hours from the antibiotic.
- For IBS symptoms: Use a multi-strain probiotic or a strain with IBS evidence (follow product RCT dose), continue for 8–12 weeks and assess symptom changes. If no benefit after an evidence-based course, stop and re-assess.
- For general maintenance / gut support: Low-to-moderate dose probiotic (e.g., 1–10 billion CFU/day) with dietary fiber and prebiotic foods; use prebiotic 1–5 g/day to start and increase gradually.
Choosing between food sources and capsules
- Fermented foods (yogurt, kefir, kimchi) provide dietary probiotics and additional nutrition; they are good first-line choices for many people. Capsules provide controlled strains and doses useful when specific evidence-backed strains are needed (e.g., AAD prevention, clinical IBS trials).
Regulation and labeling — what you need to know
- In many countries probiotic supplements are regulated as foods/dietary supplements, not medicines; therefore, efficacy claims are limited and quality varies. Look for brands that publish third-party test reports and list exact strains and CFU counts. Emerging regulatory frameworks and “live biotherapeutic products” (LBPs) may increase standards over time.
Quick decision flowchart
- Are you severely ill, hospitalized, or immunocompromised? → Talk to your doctor first (some risk).
- Are you taking antibiotics and worried about diarrhea? → Consider probiotic strains with AAD evidence (e.g., S. boulardii, L. rhamnosus GG) and follow dosing guidance.
- Do you have IBS? → Try an evidence-based probiotic for 8–12 weeks under clinician guidance.
- Want general gut support? → Improve diet (fiber + fermented foods) + optional low-dose probiotic and prebiotic, titrate slowly.
Frequently Asked Questions (short & snippet-friendly)
Q: Are probiotic capsules safe to take daily?
A: For most healthy adults, yes — they are generally safe, with mild transient GI side effects at the start. People with severe illnesses or weakened immune systems should consult their clinician first.
Q: Which probiotic strain prevents antibiotic-associated diarrhea?
A: Saccharomyces boulardii and Lactobacillus rhamnosus GG are among strains with the best evidence for preventing AAD when taken during antibiotic therapy.
Q: How long until I see benefits?
A: For acute diarrhea or AAD prevention benefits can appear within days to weeks. For IBS and metabolic effects, trials typically run 4–12 weeks. If no benefit after an evidence-based trial length, stop and reassess.
Q: Can probiotics cause infections?
A: Rarely — mostly in severely ill or immunocompromised people. For this reason, such patients should only use probiotics under medical supervision.
Q: Should I take prebiotics and probiotics together?
A: Sometimes — synbiotics pair a probiotic with a prebiotic to boost that strain’s survival and function. This can be useful but should be matched thoughtfully to the strain and clinical goal.
Bottom line / Conclusion
Prebiotic and probiotic capsules are useful tools — not magic bullets — for supporting gut health. The strongest, most consistent evidence supports probiotic use for preventing antibiotic-associated diarrhea and improving some IBS symptoms, while prebiotics reliably feed beneficial microbes and may boost mineral absorption and immune markers in specific contexts. Always pick products with clearly labeled strains, clinically supported dosing, and third-party testing; consult your healthcare provider if you are pregnant, severely ill, or immunocompromised.