Signs of Vitamin B12 Deficiency: Symptoms, Causes & Treatment
Vitamin B12 — also called cobalamin — is a water-soluble vitamin critical to blood formation, nervous system health, and DNA synthesis. Because the body stores B12 in the liver, deficiency often develops slowly and may be overlooked until symptoms are clear. This guide explains what B12 does, how deficiency shows up (early and severe signs), the main causes, how clinicians test for it, treatment approaches, and the best food sources.
What B12 does in the body
Vitamin B12 is required to:
- make healthy red blood cells (preventing megaloblastic anemia),
- maintain myelin (the insulating sheath around nerves), and
- support normal DNA and neurotransmitter synthesis.
When B12 is low, red blood cells may be fewer and abnormally large (megaloblastic anemia), and nerves may lose normal function — producing sensory symptoms, balance problems and, if untreated, permanent damage.
Early symptoms
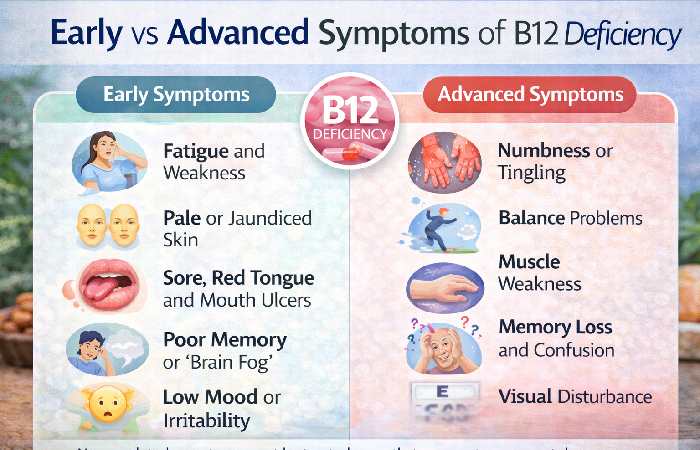
Early B12 deficiency can be subtle and non-specific, which is why it’s often missed. Look for:
- Fatigue, weakness and low energy. The oxygen-carrying capacity of blood falls as anemia develops, producing tiredness.
- Pale or slightly jaundiced skin. Breakdown of abnormal red cells may cause mild yellowing.
- Sore, smooth or red tongue (glossitis) and mouth ulcers. This is a classic early sign.
- Appetite loss, weight loss, or mild gastrointestinal upset. Some people report nausea or diarrhea.
- Mild cognitive or mood changes. Low B12 is associated with poor concentration, “brain fog,” low mood or irritability.
Because these symptoms overlap with many other conditions, clinicians use risk factors and tests to decide whether to check B12 levels.
According to the Cleveland Clinic overview of vitamin B12 deficiency symptoms, early signs may include fatigue, appetite loss, mouth ulcers, pale skin, and neurological symptoms that worsen gradually if untreated.
Severe (advanced) symptoms — neurological “red flags”
If deficiency progresses, neurological damage can occur and may become irreversible if therapy is delayed. Advanced signs include:
- Paresthesia: Numbness, tingling, or “pins and needles” in hands and feet.
- Gait disturbance and balance problems: Loss of proprioception (position sense) and vibration sense can cause unsteadiness.
- Coordination and weakness: Difficulty walking, falls, or limb weakness in severe cases.
- Memory loss, confusion or dementia-like symptoms: Especially in older adults; cognitive decline may not fully reverse if treatment is very late.
- Visual disturbances: Optic nerve involvement can lead to blurred vision.
Important clinical point: Neurological signs should trigger urgent evaluation and prompt treatment because permanent damage is possible. Guidelines emphasise not delaying treatment while waiting for test results when neurological symptoms are present.
Causes of vitamin B12 deficiency
B12 deficiency results from any of three broad problems: low intake, impaired liberation/absorption, or impaired transport/use.
1. Low dietary intake
- Strict vegan or vegetarian diets without fortified foods or supplements are a common cause because B12 is naturally found in animal products. Infants of vegan mothers are especially at risk.
2. Impaired absorption/intrinsic factor problems
- Pernicious anemia (autoimmune destruction of stomach cells that make intrinsic factor) prevents absorption of dietary B12 and is a classic cause; it often requires lifelong replacement.
- Post-surgical patients: Removal of portions of the stomach or ileum (some bariatric procedures) reduces absorption.
- Chronic gastritis or atrophic gastritis reduces acid and intrinsic factor production.
3. Malabsorption from intestinal disease or infections
- Celiac disease, Crohn disease, certain intestinal infections or bacterial overgrowth can impair uptake.
4. Medication-related
- Metformin (used for diabetes) and proton pump inhibitors / H2 blockers (used for reflux) reduce absorption in some people when used long-term. Nitrous oxide (laughing gas) inactivates B12 and can precipitate deficiency.
5. Increased requirement or other
- Pregnancy, breastfeeding, and some chronic illnesses may increase needs or reveal marginal status.
Tests and diagnosis
Diagnosing B12 deficiency usually starts with blood tests and clinical evaluation.
Initial tests
- Complete blood count (CBC): may show macrocytic (large) red blood cells and low hemoglobin/hematocrit, but early deficiency can exist without anemia.
- Serum total B12 (cobalamin): common screening test; low values suggest deficiency but borderline results are common.
More specific tests (when needed)
- Methylmalonic acid (MMA): rises when intracellular B12 is low and is a sensitive marker for deficiency.
- Homocysteine: also rises in B12 (and folate) deficiency but is less specific.
- Holotranscobalamin (active B12): newer test showing available B12 fraction.
- Intrinsic factor antibodies and parietal cell antibodies: useful when pernicious anemia is suspected.
Interpretation tip: “Low serum B12” is not the whole story — clinicians combine symptoms, risk factors, and MMA/holoTC to confirm deficiency. NICE and other guidance note that some people with symptoms but borderline serum B12 should be further assessed rather than dismissed.
Treatment options
Treatment aims to restore B12 stores and reverse symptoms — faster for blood abnormalities than for neurological recovery.
Clinical resources such as the Mayo Clinic guide to vitamin deficiency anemia diagnosis and treatment explain that treatment typically involves vitamin B12 supplementation through injections, oral tablets, or nasal formulations depending on the underlying cause.
1. Intramuscular (IM) injections — when to use
IM cyanocobalamin or hydroxocobalamin is the traditional route and is preferred when absorption is impaired (pernicious anemia, post-gastric surgery) or when neurological symptoms are present because it bypasses the gut. Typical regimens (examples used in practice/guidelines):
- Loading phase: 1000 µg (1 mg) IM daily or alternate days for 1–2 weeks (regimens vary).
- Maintenance: 1000 µg IM every 1–3 months lifelong if cause irreversible (e.g., pernicious anemia).
NICE and other guideline summaries emphasise prompt parenteral therapy for neurological signs and that treatment should not be delayed while awaiting tests.
2. High-dose oral therapy
High-dose oral cyanocobalamin (e.g., 1000–2000 µg daily) can be effective even when intrinsic factor is absent because a small proportion (~1%) is absorbed by passive diffusion at very high doses. Oral therapy works well for dietary deficiency or in patients who can reliably absorb and adhere to treatment. For some patients, daily high-dose oral therapy is an alternative to injections.
3. Nasal or sublingual preparations
Nasal gels and sublingual tablets exist and may be useful in maintenance for some patients, though availability and cost vary.
4. Duration of therapy
- If the cause is temporary (dietary), treatment continues until levels normalize and the cause is corrected, then maintenance or dietary advice suffices.
- If the cause is permanent (pernicious anemia, major GI surgery), lifelong replacement is usually required.
Monitoring response
- Hematologic response (reticulocyte count) often rises within 3–7 days; anemia usually improves in weeks.
- Neurological recovery may take months and sometimes remains incomplete — earlier treatment gives better outcomes.
- If symptoms do not improve, clinicians re-check adherence, re-measure MMA/homocysteine, and consider alternative diagnoses.
Foods rich in vitamin B12
Because B12 is mostly in animal products, diet advice is key for prevention:
- Shellfish (clams, oysters), fish (salmon, tuna), beef liver — among the richest natural sources.
- Meat, poultry, eggs, milk and dairy — regular sources for omnivores.
- Fortified foods — many plant milks, breakfast cereals and nutritional yeast are fortified and valuable for vegetarians/vegans.
Practical tip: Vegans should take reliable B12 supplements or consume fortified foods daily; breastfeeding vegan mothers should ensure adequate intake to protect infants.
Who should be tested?
Consider B12 testing in people with:
- symptoms listed above (especially neurological),
- risk factors: vegans, older adults (>65), history of gastric surgery, chronic PPI/metformin use, autoimmune disease, or unexplained macrocytic anemia.
Preventing deficiency
- Eat B12-rich foods or use fortified products.
- If you take long-term metformin or acid-suppressing drugs, discuss B12 monitoring with your clinician.
- Older adults and those with absorption risk factors may benefit from periodic B12 checks.
- Pregnant or breastfeeding vegans should plan B12 supplementation.
FAQs
Q — Can B12 deficiency cause depression or memory loss?
A — Yes. Low B12 is associated with mood changes, depression and cognitive symptoms; treatment can improve some cognitive features, especially if started early.
Q — Is a low serum B12 always diagnostic?
A — No. Serum B12 can be borderline; MMA and holotranscobalamin are often used to clarify true deficiency.
Q —Which is better: injections or oral B12?
A — It depends: injections are preferred for absorption problems or neurological symptoms; high-dose oral therapy can be effective for dietary deficiency and some patients with absorption issues because of passive diffusion. Discuss with your clinician.
Q —Can B12 overdose occur?
A — B12 is water-soluble and generally safe; toxicity is extremely rare at usual supplement doses. Follow clinical advice if you have specific health conditions.
Practical patient checklist
- Note symptoms and risk factors (diet, meds, surgeries).
- Book a GP visit and request CBC + serum B12.
- If serum B12 is low or borderline with symptoms, ask about MMA/holoTC tests.
- If neurologic signs are present, seek urgent assessment — treatment should not be delayed.
Final note
This article is informational and not a substitute for medical care. If you or someone else has neurological symptoms (numbness, weakness, balance problems), severe fatigue, or signs of anemia, seek medical attention promptly — early diagnosis and treatment are key to preventing irreversible nerve damage.